BREAKING NEWS
Launching 1st March 2023. Also check out: https://www.thailandmedical.news/
The number of adult patients with congenital heart disease is growing worldwide.
Advances in medical treatment, percutaneous interventions, and surgery offer the vast majority of these patients a good life expectancy. However, life long follow-up is needed, especially for patients with residual lesions or sequels of previous interventions.
This is why several adult congenital heart disease centers were set up. Although these centers initially aimed at providing optimal medical care, they also started to fulfill the need of these patients for including socio-professional counseling, socio-juridical help, and advice on physical activity.
Indeed, it has been shown that physical activity in patients with congenital heart defects does not only improve their exercise capacity, but has also a beneficial effect on the mental health status.
However, some studies showed that young patients with congenital heart disease tend to be more obese, which seems to be related to a more sedentary lifestyle.
It is not uncommon that families overprotect some patients. But, also counseling physicians are not always sure about the type and the intensity of the exercise that could be allowed.
In contrast, there are patients who want to exert themselves to limits that would better be avoided. So, the balance between under- and overprotection to maximize the benefit and to minimize the risk of physical activity has to be found for each individual.
Several guidelines and recommendation papers have been published over the last years. However, applying these in daily practice discovered shortcomings and is maybe the reason why it is not uncommon that different sport advices are proposed for the same patient.
The ESC recommendations on competitive and elite sports can’t be used, because they would be too restrictive for the overall adult congenital heart disease population.
Other recommendations focus on children so that extrapolating them uncritically to adolescents and (young) adults would be wrong.
Finally, in all papers on sport counseling the decision taking process is based on the anatomical defect. This leads to an unpractical long list of congenital heart defects that might have in their turn a variety of hemodynamic and electrophysiological sequels.
For example, the exercise performance of a patient with repaired atrial septal defect without pulmonary arterial hypertension will differ from a patient with a repaired atrial septal defect with pulmonary arterial hypertension.
The exercise performance of a patient with a repaired tetralogy of Fallot and severe pulmonary valve regurgitation with normal right ventricular function will differ from a patient with a repaired tetralogy of Fallot and severe pulmonary valve regurgitation with a severely damaged right ventricle.
Because of the variety of anatomical and functional differences in these patients the idea arose to start the decision tree from the actual hemodynamic and electrophysiological status of the patient.
This new concept and the lacking recommendations for adolescents and (young) adults motivated the Working Group of Grown Up Congenital Heart Disease and the Section on Sports Cardiology for writing a position paper.
The scope was to produce clear, concise and practical recommendations, which can be used as an everyday clinical tool by congenital heart disease specialists.
The recommendations would cover a wide spectrum of physical exercise, ranging from everyday physical activity to participation in leisure time sports. A six steps approach was developed.
The first step is the review of the history of the patient, to understand the underlying congenital heart defect, and to know its potential complications. Alarming symptoms must first be worked out before and the clinical examination has to fit with the underlying disease.
By the second step, five functional parameters are assessed:
Evaluating these five variables gives insight in the hemodynamic and electrophysiological status of the patient. Dependent on the deviation from normal values, which are predefined in the position paper, the patient will enter the algorithm through a different route (Figure).
In the third step is decided on the static component of the exercise. The basic idea is protecting the pressure or volume loaded ventricles and the aorta from the static component of an exercise. For example, for a moderate aortic valve stenosis, physical activity with a moderate static component is proposed (Figure).
The fourth step is the (cardiopulmonary) exercise test. Based on the Borg scale and/or the maximal heart rate achieved during the exercise test, it is possible to delineate for each individual the level for “high” intensity, “moderate” intensity, and “low” intensity of an exercise.
Dependent on the hemodynamic and electrophysiological status of the patient, the static component of an exercise is proposed. The level of intensity is decided on following the algorithm (Figure, solid lines) in step five.
However, the algorithm may not be interpreted too restrictive. If a patient wants to sport with a higher static component, whereas the position paper suggests physical activity with a lower static component, it is suggested to perform at a lower intensity.
For the frequency and duration of each exercise session, a combined minimum of 3 to 4.5 hours of physical activities per week is recommended; the minimum minutes per session should be 30 minutes. For team sports patients should be encouraged to participate in teams (or with peers) of similar physical fitness.
The sixth step is follow-up. For patients training regularly at high intensity, follow-up as indicated by the ESC guidelines for competitive and elite sports is proposed. For patients with physical activities at moderate or low intensity level, follow-up as suggested by the ESC guidelines for grown up congenital heart disease is proposed. However, when signs or symptoms change, the patient needs to reenter the algorithm at step one.
To conclude the position paper envisages that these recommendations will result in more unified physical activity protocols.
Such an individualized exercise prescription might offer a platform with the aim to maximize benefit for health and minimize the cardiovascular risk.
Finally, it could be used as a tool for future research to increase the lacking level of evidence.
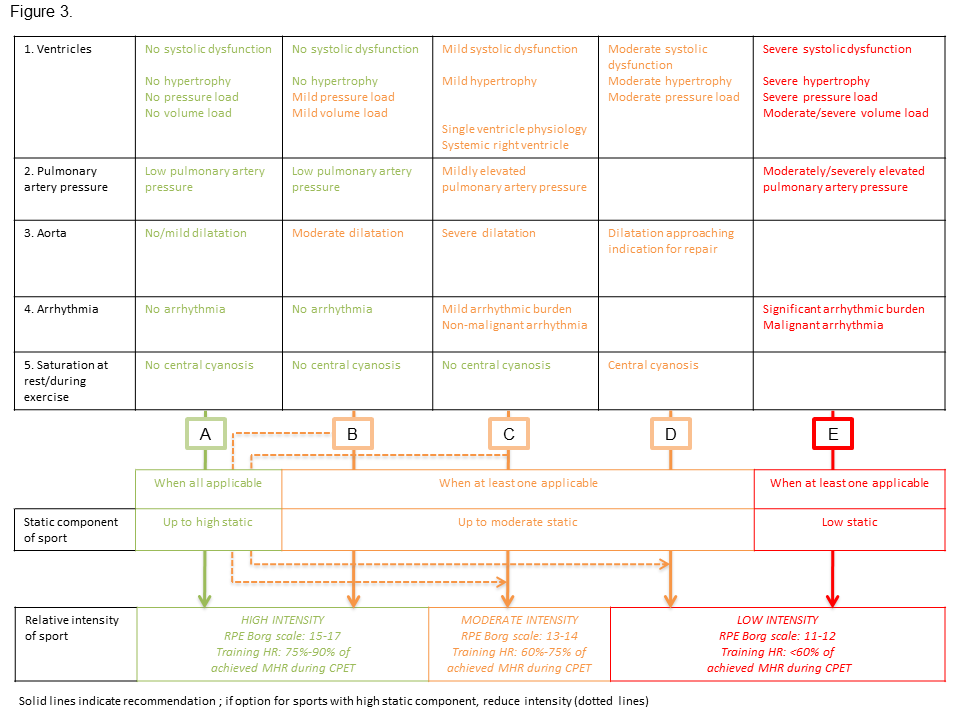
Figure. (Click Image for larger view) Flow chart depicting in detail steps 2 to 5. Following evaluation of the five variables and the interpretation of the CPET, an individualized recommendation can be provided (solid lines). When patients insist on sports with high static component, where it is not recommended, PA at a lower level intensity is suggested (dotted lines).
Physical activity in adolescents and adults with congenital heart defects; individualized exercise prescription.
Budts W, Börjesson M, Chessa M, van Buuren F, Trigo Trindade P, Corrado D, Heidbuchel H, Webb G, Holm J, Papadakis M.
Eur Heart J. 2013 Nov 7 doi:10.1093/eurheartj/eht433