BREAKING NEWS
Launching 1st March 2023. Also check out: https://www.thailandmedical.news/
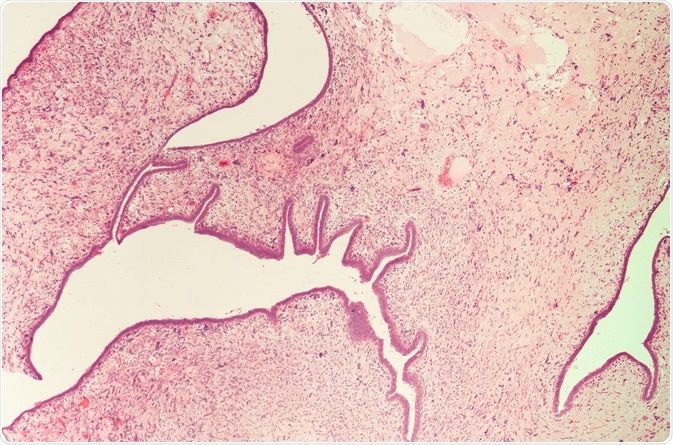
Phyllodes tumors are unusual tumors of the breast that begin their growth in the connective tissue of the breast. These tumors occur most often in females who are 30 to 40 years of age, although they might be found in women who are either older or younger. They account for less than 1% of all breast tumors.
Not often, in about 10% of cases, these tumors can be cancerous. When cancerous, there is an approximate 25% chance that phyllodes tumors of the breast will be metastatic. In these instances, a patient essentially has a fatal diagnosis - long-term survival is rare.
Moreover, phyllodes tumors have unusual behavior - their growth cannot always be predicted. Based on their microscopic structure, they are different from other malignant tumors as they contain epithelial elements within their connective tissue.
Most often, a lump in the breast will indicate the existence of a phyllodes tumor. While not painful, it can be easily felt by gynecologists when examining the breasts. Tumor growth is rapid, with its size reaching 3cm or larger often within several weeks. The speed of growth does not necessarily mean that the tumor is cancerous.
The lump eventually will appear as a bulge in the skin. In some instances, whether benign or cancerous, the existence of these tumors may form an open wound on the skin of the breast, or may cause an ulcer to appear.
Because physicians do not see phyllodes tumors often, they may not recognize them as such and face difficulty diagnosing them. It may also prove challenging for clinicians to differentiate these tumors from fibroadenomas on imaging tests. This is because they are similar in appearance to fibroadenomas, which are common benign growths, especially among younger women.
Two key differences between fibroadenomas and phyllodes tumors are that the tumors tend to grow more quickly and develop in women who are in their 40s as opposed to their 30s. These differences can help doctors distinguish phyllodes tumors from fibroadenomas. Usually, the complete tumor must be removed for diagnosis to determine whether it is indeed a phyllodes tumor, and whether it is cancerous.
The actual diagnosis may entail:
A diagnosis would be more definitive if an excisional biopsy is performed, in which the entire abnormality is removed.
Most often, phyllodes tumors are surgically removed as the primary treatment approach. A total mastectomy may be required. Cancerous phyllodes tumors are different from cancer of the breast. Hormonal therapy usually does not bring beneficial results. In addition, the tumors probably will not respond well to radiation nor chemotherapy regimens.
After surgery, because of the strong potential of tumor recurrence, patients have been treated with adjuvant radiotherapy. Research has shown that those who received adjuvant radiotherapy would encounter less of a risk of local tumor recurrence. Unfortunately, the results have not been consistent.
An examination of research indicated that adjuvant radiotherapy for tumors, which were either classed as borderline cancerous or cancerous, lessened the rate of local recurrence in those patients who had breast conserving surgery. Yet, radiotherapy did not have any impact on a patient’s overall survival or disease-free survival outcome. Multicenter prospective randomized controlled studies with extensive followup periods and well defined parameters may be required to clarify the effectiveness of adjuvant radiotherapy.
It appears that adjuvant chemotherapy does not have an established benefit in phyllodes tumors either. There has not been any double blinded, multicenter study undertaken, however one observational study did occur over a 10 year period. In this research, patients were administered doxorubicin in combination with dacarbazine or observation alone after surgery.
Limited data indicated that one option could involve offering adjuvant chemotherapy to patients who have repeating larger-than-5-cm sized cancerous tumors. A better understanding of this option would be first required, possibly by evaluating adjuvant chemotherapy for cancer of the soft tissue. Other investigators have shown that doxorubicin- and ifosfamide-based chemotherapies may be somewhat effective against cancerous phyllodes tumors.