BREAKING NEWS
Launching 1st March 2023. Also check out: https://www.thailandmedical.news/
Solar or actinic elastosis is a condition associated with chronic ultraviolet damage superimposed on aging skin. It presents as a yellowish thickened appearance to the skin which is bumpy and covered with furrows.
The condition is due to the accumulation of disordered elastic tissue in the upper and middle layers of the dermis, which are most susceptible to sun exposure. In this way solar elastosis is a biological indicator of the degree of ultraviolet-induced skin damage the individual has sustained, being a protective or compensatory response.
Long-term exposure to sunlight is the best-known risk factor for solar elastosis, with all skin types being equally affected. Smoking is another established risk factor, because it encourages the production of tropoelastin fibers and the degradative enzymes matrix metalloproteinases (MMP).
These break down the matrix and result in disorderly elastin arrangement within the skin layers. The damage to the skin is restricted to the superficial papillary dermis in cases of photoaging, whereas tobacco smoke exposure produces deeper damage penetrating into the reticular dermis.
People with light skin and blonde hair, or light eyes, are especially prone to developing actinic keratosis if they are living in a sun-drenched climate and are exposed to the outdoors for a long period. This is also associated with the rapid development of freckles or sunburn following sun exposure. Immunocompromised individuals are more vulnerable to this type of skin damage as well.
Solar elastosis causes few signs or symptoms other than a slowly enlarging patch of reddish skin, first appearing after the age of 40 years. It is bumpy or rough to the surface, and may be associated with an itching or burning sensation.
These lesions appear first on the sun-exposed areas of the skin, such as the face and lips, the ears, the neck and the forearms or hands. In older people, elastosis may eventually increase the risk of melanoma of the skin.
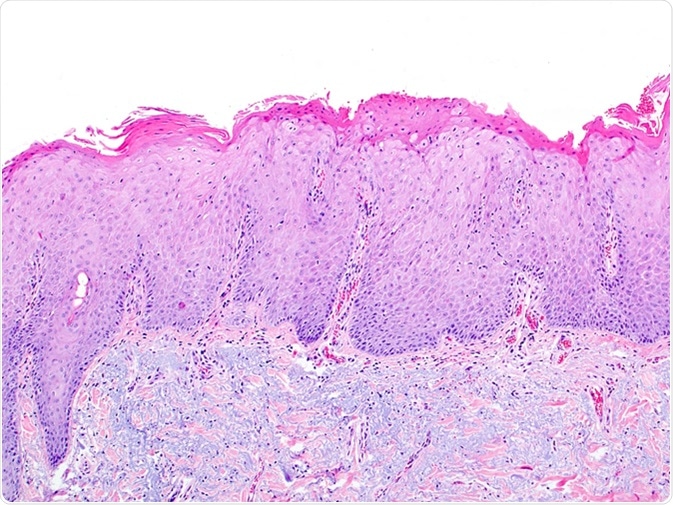
The diagnosis of solar elastosis is clinical supplemented by biopsy from the affected area. This shows loss of eosin staining in the upper skin layers resulting in a blue stain, with the appearance of grossly disorganized elastin fibers in the dermis. Treatment should be timely.
It may be possible to improve the cosmetic appearance of the elastotic skin using laser ablation, botulinum toxin injections to reduce nervous activity and relax the skin, dermal fillers to fill in the contours and reduce the depth of the furrows, and topical imiquimod.
In the long run, some of these lesions but not the majority may develop into a form of skin cancer called squamous cell carcinoma. This is also a curable form of cancer if caught early, and so any change in a solar elastosis lesion should be taken seriously and screened by a dermatologist. A yearly screening is advisable in all cases.
Solar elastosis can be prevented by: